Peer-Reviewed Evidence
The science is not ambiguous.
Treatment plan at Preval Health is grounded in landmark clinical trials and consensus statements published in the highest-impact medical journals. This is not alternative medicine. This is the frontier of evidence-based cardiology.
Foundational Evidence
The evidence speaks for itself.
Prescription cholesterol management saves lives that diet and exercise alone cannot. The evidence is published, peer-reviewed, and reproducible.
Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights
Borén J et al. · European Heart Journal (2020)
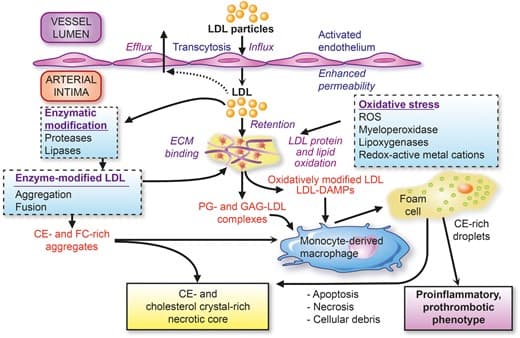
LDL is the principal driver of atherosclerosis. Treatments that reduce LDL-C lead to fewer cardiovascular events, and aggressive lowering stabilizes plaques by increasing collagen content and reducing lipid accumulation and inflammation.
This EAS Consensus Panel statement consolidates pathophysiological, genetic, and clinical trial evidence confirming that LDL particles cause atherosclerotic cardiovascular disease. The relationship is causal and dose-dependent. Lowering LDL-C with statins, ezetimibe, and PCSK9 inhibitors produces favorable plaque modifications. The panel also highlights the emerging role of other ApoB-containing lipoproteins, including Lp(a), in driving residual cardiovascular risk.
Read full paper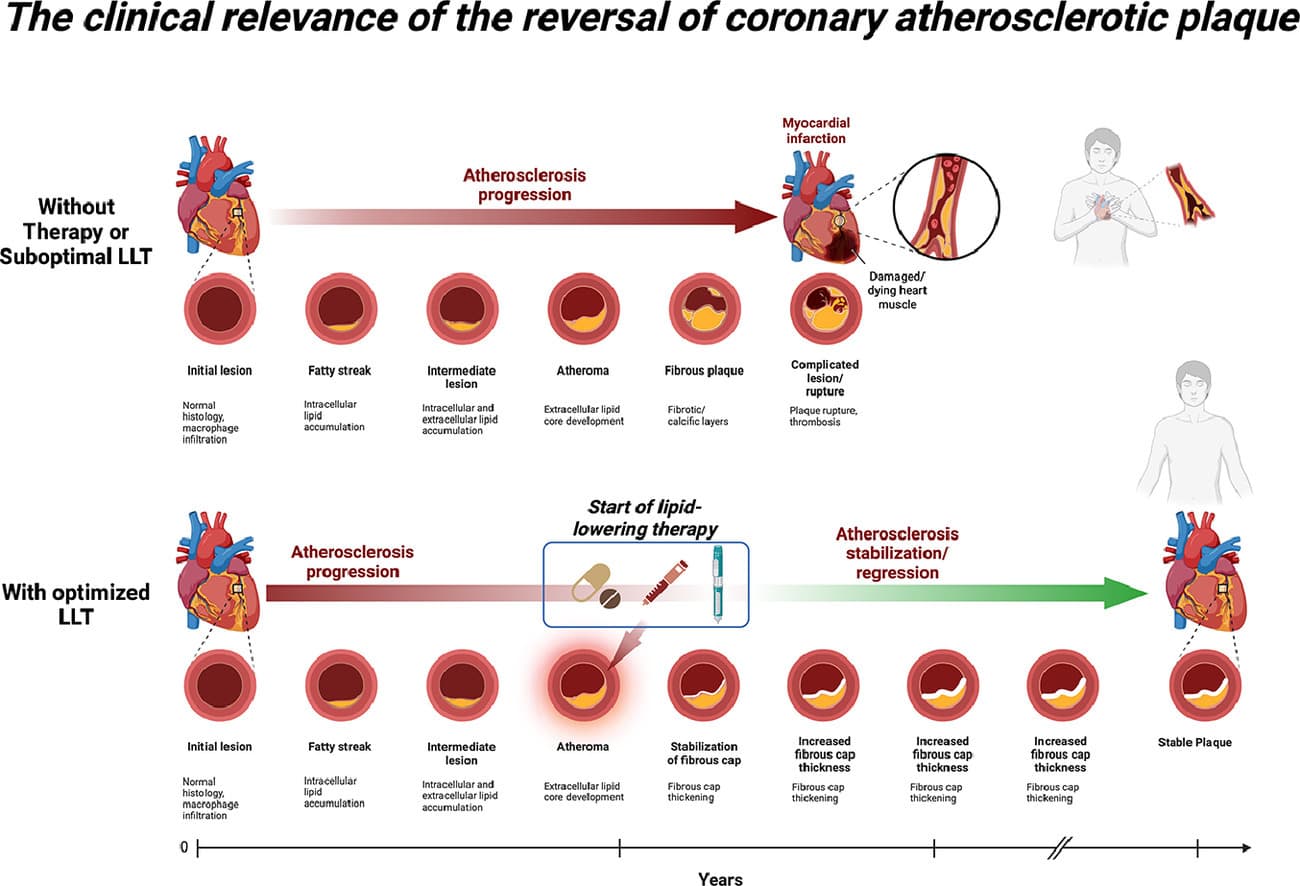
The Clinical Relevance of the Reversal of Coronary Atherosclerotic Plaque
Cesaro A et al. · European Journal of Internal Medicine (2024)
Intensive lipid-lowering therapy induces measurable plaque regression: reducing plaque volume and improving plaque composition. Plaque stabilization or regression is the phenomenon linking LDL-C reduction to fewer cardiovascular events.
This 2024 review consolidates evidence from IVUS, OCT, and NIRS imaging studies showing that aggressive LDL-C lowering with statins and PCSK9 inhibitors can physically reverse coronary plaque buildup. The top pathway shows what happens without treatment: plaque progresses from fatty streak to rupture and heart attack. The bottom pathway shows what happens with optimized lipid-lowering therapy: plaque stabilizes, the fibrous cap thickens, and progression halts. The connection between lower LDL-C and fewer heart attacks is not abstract. It is visible on imaging.
Read full paper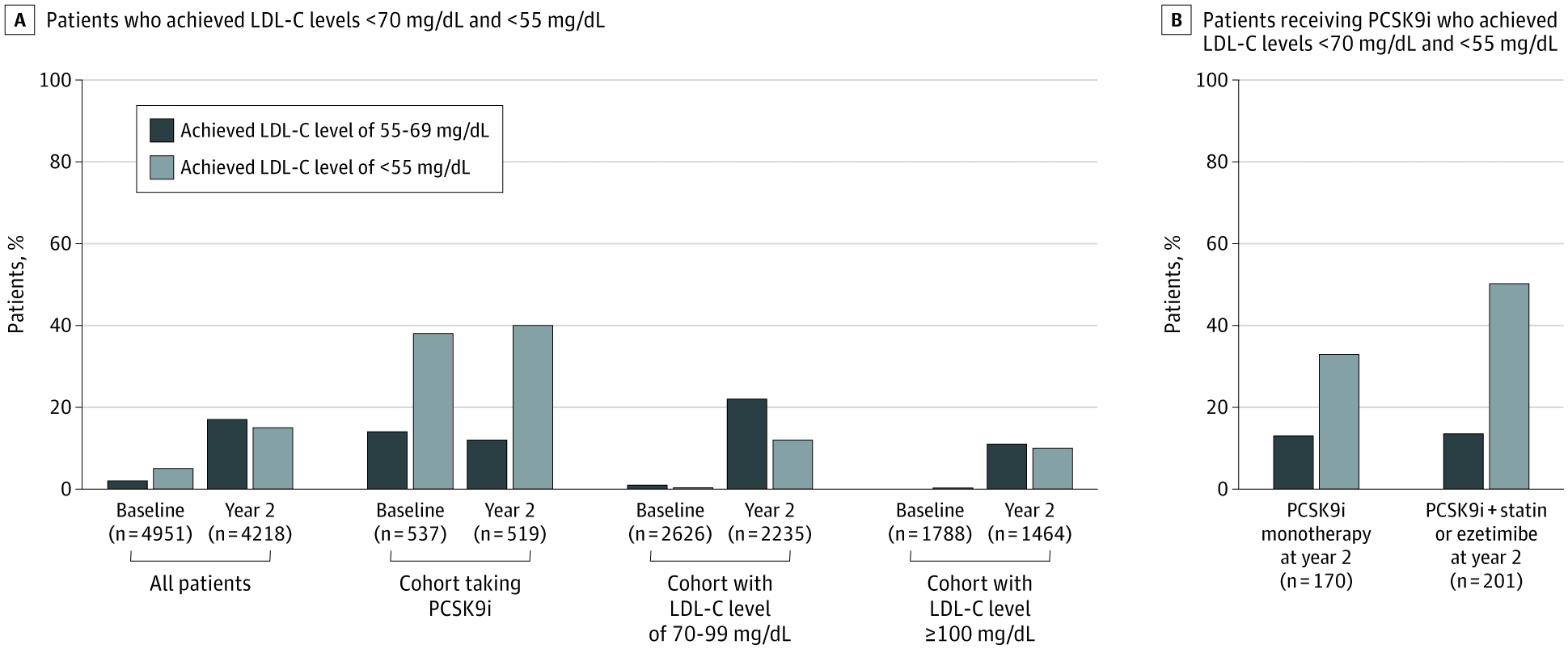
Use of Lipid-Lowering Therapies Over 2 Years in GOULD, a Registry of Patients With Atherosclerotic Cardiovascular Disease in the US
Nelson AJ et al. · JAMA Cardiology (2021)
Among US patients with ASCVD not on a PCSK9 inhibitor, only 44% were on high-intensity statins and just 9% were on ezetimibe. Fewer than 1 in 5 high-risk patients achieved an LDL-C below 70 mg/dL.
The GOULD registry tracked lipid-lowering therapy use across US clinical sites in patients with established atherosclerotic cardiovascular disease. At 2 years, only 21% of the highest-risk patients achieved guideline-recommended LDL-C levels. PCSK9 inhibitors - proven to regress plaque - were prescribed to a negligible fraction. The medications exist. The evidence is unambiguous. The prescriptions are not being written.
Read full paper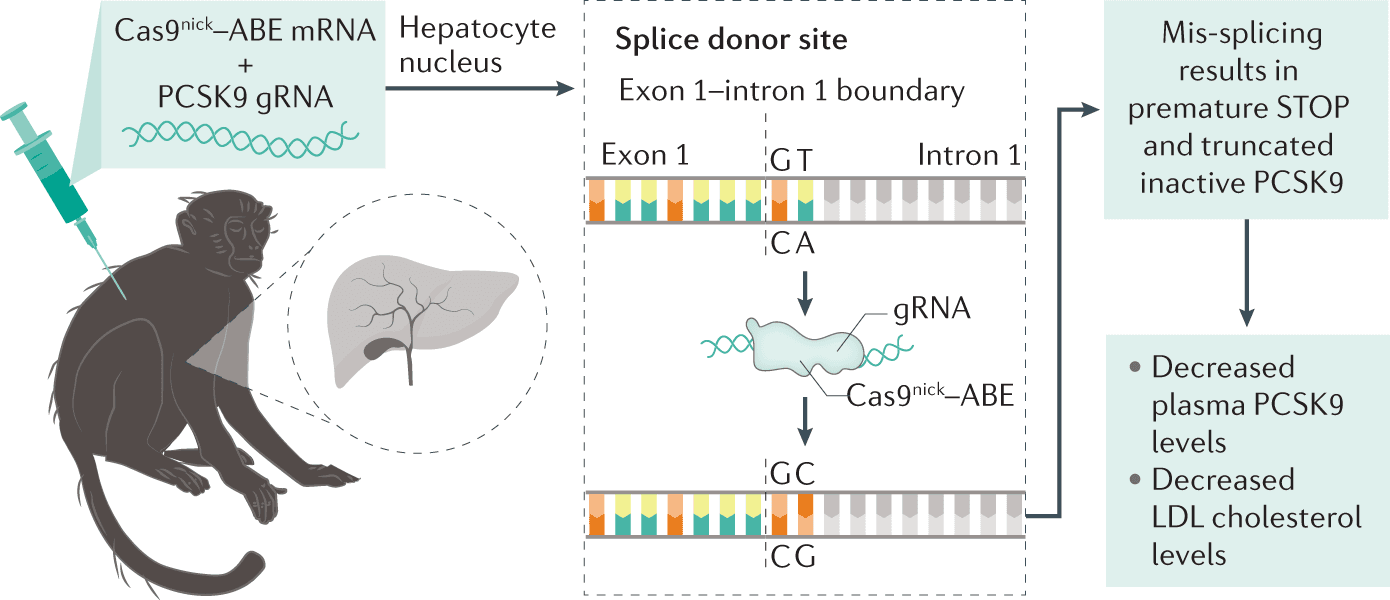
In vivo CRISPR base editing of PCSK9 durably lowers cholesterol in primates
Musunuru K et al. · Nature (2021)
A single infusion of adenine base editor targeting PCSK9 reduced LDL-C by ~60%, sustained over 8 months.
Using lipid nanoparticle-delivered adenine base editing in cynomolgus monkeys, a single infusion reduced circulating PCSK9 protein by approximately 90% and LDL-C by approximately 60%, with effects durably maintained for at least 8 months. This proof of concept from Verve Therapeutics demonstrates that a one-time treatment could permanently eliminate the need for ongoing cholesterol medication.
Read full paperTherapeutic Pipeline
What's coming next.
The next generation of cardiovascular therapies is in clinical trials now. From twice-yearly injections to one-time gene edits, the future of cholesterol management is arriving faster than guidelines can keep up.
Lepodisiran
A small interfering RNA that silences hepatic Lp(a) production. Lp(a) is a genetically determined, independent cardiovascular risk factor that no existing approved therapy can meaningfully lower.
Key Result
A single dose reduced Lp(a) by up to 96% from baseline, with reductions sustained for up to 48 weeks at the highest dose.
Muvalaplin
The first oral small-molecule inhibitor of Lp(a) assembly. It disrupts the apo(a)-apoB100 interaction, preventing Lp(a) particle formation entirely.
Key Result
Reduced Lp(a) by up to 65% in a phase 2 trial - the first time an oral agent has achieved meaningful Lp(a) reduction.
Inclisiran
A synthetic siRNA targeting PCSK9 mRNA in hepatocytes, delivered as a subcutaneous injection twice yearly. Already approved as Leqvio.
Key Result
Reduced LDL-C by approximately 50% versus placebo with just two injections per year in the ORION-10 and ORION-11 trials.
VERVE-101
A single-infusion gene editing therapy that permanently inactivates PCSK9 in the liver via adenine base editing delivered by lipid nanoparticles. One treatment. Lifetime effect.
Key Result
Early human data showed a single infusion reduced blood PCSK9 by up to 84% and LDL-C by up to 55% in patients with familial hypercholesterolemia.
Verve Therapeutics, AHA 2023 · AHA Scientific Sessions (2023)
Pipeline therapies shown are based on published clinical trial data and may not yet be available for prescription. Preval Health prescribes only FDA-approved medications. We monitor the therapeutic pipeline to ensure our patients benefit from advances as soon as they become clinically available.
The evidence exists. The therapies exist.
The only question is whether you have access to a clinician who will use them. That is what Preval provides.
Join the Waitlist